 Live Music Archive
Live Music Archive Librivox Free Audio
Librivox Free Audio Metropolitan Museum
Metropolitan Museum Cleveland Museum of Art
Cleveland Museum of Art Internet Arcade
Internet Arcade Console Living Room
Console Living Room Books to Borrow
Books to Borrow Open Library
Open Library TV News
TV News Understanding 9/11
Understanding 9/11tv Key Capitol Hill Hearings CSPAN March 5, 2014 4:00am-6:01am EST

























































4:59 am

>> it is only appropriate everybody take your telephone device and take a photo of yourself. [laughter] because anybody that would
5:00 am

start a meeting before a:00 on the eastern time zone cannot be all there. i am assuming that most of you had the opportunity to get at least your first cup of $10 starbucks down your belly and feeling good. good morning. first of all, i want to make knowledge somebody before you yesterday. fit campbell for the job he did 2013 the passion and disorganization for our industry has been incredible and part of what this is all about is the type of person that vic is the effort is a guiding light for those of us that will have to follow
5:01 am

me with all the things that he did. please stand up everybody give him a round of applause [applause] ladies and gentlemen, this morning i was supposed to be sharing the stage with jim the chairman of the american hospital association and president and ceo of presbyterian health services n new mexico. he was supposed to be here with us but unfortunately the weather eliminated his ability to make it. the reason he was going to be here is we are fierce competitors in in new mexico and it just happened in being the chairman of the hospital association and the of the federation we thought we would have a good time up here today to talk and banter but unfortunately he could not make it so we will
5:02 am

have to share the stage together another time. but even without him we will still have the especially valuable time for all of us. as we hear directly from the political and policy leaders who would shape and impact on industry in the months and years to come, from the comments i have heard yesterday this meeting is already a success for many of you. i heard you talk about the you a bite to get a big bottle of scotch to sit down with the generals with -- for two hours to find out what he really knows. [applause] but also about the buyers exposition i had the opportunity to walk through the halls this today at lunch and none of you were there.
5:03 am

[laughter] they q for your role with the success of this exposition and a special thanks to our sponsors their names will be scrolling across the screen hoping to take the opportunity to a knowledge who they are. i have been to this event for about 25 years. it seems odd i remember the cherry blossoms blooming. it may be later but there is a stark difference to what is going on today that it is about 16 degrees versus when there was so much pollen in the air you could hardly breathe. but think of the transition from the winter to spring we continue to be in transition. but we are not the only industry that always goes
5:04 am

through a transition. whether banking or the opposite may be the video industry. how many of you out there today think three years or five years ago had a card in your pocket and it was a blockbuster card. how many had one? on the views still do? [laughter] they are taking up space if you still have one today. by blockbuster was a dominant leader in that industry. but it was capital intensive , brick and mortar and employees. then this organization netflix comes up the business model was a little different. was capital, a large
5:05 am

distribution centers and few were employees. then they introduce streaming video to cut more capital to do more with their employees. them last week they announced a big deal with comcast to get directly to the cable customer to deliver even faster speeds. during the hours of netflix subscribers generate 30% of the downloading activity on the internet. between nine and 11:00 p.m. 30 percent of that activity goes through netflix video. that is expected to continue to increase with the comcast transaction. all this was was a simple
5:06 am

disruptive transition one business model going to another. for us whether the affordable care act or all the other things there is a great deal of uncertainty as we begin our own transformation with tremendous financial and operational pressures brought on this by the largest player, the federal government and a much more powerful customer. the best ideas all come from washington d.c. if you don't believe me ask them. [laughter] . .
5:07 am

we have all the same cost better paid one-third of what we used to. that's not right. but that is what is happening to our hospitals. ladies and gentleman for those of you in this room that are suppliers, vendors and partners of our hospital
5:08 am

, the more money they take from us the less money we have to spend with you. as we continue to educate policy leaders regulations don't make sense. . .
5:09 am

this notion that medicare is that the bank for every other program that lacks funding is not the solution. our industry was asked, our industry was asked to provide better services to medicare customers. we have done that. our industry was asked to improve our quality. if you look at our core measures, our hospital conditions, readmission rates, everything has improved. we did what they asked. we were asked to improve efficiencies. he looked at the facilities and operations today, we did what they asked. rearrested take cuts to help fund the four will carry act. ladies and dillon, we did that as well. please take the time to write or visit your congressional representative and let them know that there actions have consequences.
5:10 am

those consequences to our industry can be devastating if done the wrong way. i encourage you to access the federation blog which is up right now and twitter accounts, and if you need information as it relates to providing a congressional leaders with information about what their actions are doing to our industry, i would encourage you to check our blog, check the quick twitter. people will get back to you and provide blue in the information necessary, and we can educate those individuals that adversely impacting as today. we will have a great rest of the day and i would like to introduce the presidency of the federation. >> thank you, david. that was great.
5:11 am

regulators are of the morning. good morning to everyone in the audience. thank you for coming. senator, our first speaker is on the way. i want to wish you a good morning. i also remind you, as david just did, follow us on twitter and fe damer hospital. or on my twitter. also, go to an oblong. we have a terrific program this morning. i do have one thing to say. unfortunately our congressman ryan was caught in the weather, one of our casualties comanche is actually in a planner now. we're going to miss him, but he is promised that he will come next year. i'm sure all of you will be here next year, and we will have congressman ryan for you, but will beat you have is a new chairman ron wyden, senator
5:12 am

blonde, md. taverner, cms administrator and sinister to me it will be up this morning. before we get to the program i want to make an announcement, you need for this program. provides an opportunity. today we can put up the slide, today is budget day in washington. it is the day at the white house release is the president's budget for fiscal year 2015. the federation is releasing a new report on this day on national spending trends in health care, and its implications for medicare policy and the federal budget. this report was prepared by a health economist alan dobson updating a previous report that al did for us in june 2013. dobson examined the forces
5:13 am

driving the historic trends of health care growth and developed estimates of potential additional savings in medicare if the current trends continue. it has been less than a year now, but much has happened since that last report. there are new, empirical studies and new cms data. most importantly there are new congressional budget office analysis and budget forecasts. all of these are documented in that dobson report. taken together, this new information gives us even greater confidence that the force is transforming healthcare finance and delivery are structural and systematic. initially some suggested the slowdown was fueled by cyclical economic activity driven by the great depression -- great recession. although i'm sure some of like it was a great depression. new economic research suggests that the economy may have had an
5:14 am

even smaller impact on health care spending than earlier felt. the report that we were released showed that sustained slowdown is adorable and additional savings are more likely to materialize but even as the economy continues its recovery. let's go to the numbers. i will start with the punch line . $900 billion in additional medicare savings is within reach if we stay the course. what do i mean, and what does this chart show? medicare spending per beneficiary, medicare beneficiary has slowed beyond anyone's expectations and has remained low for several years. this led to a cbo, the congressional budget office lowering its annual 10-year forecast a medicare program spending for the sixth consecutive year. the cbo most recent budget
5:15 am

forecast issued last month lowered medicare spending by another $154 billion beyond its previous forecast which it issued just nine months ago. many may know that several years ago i was staff director of the house ways and means health subcommittee. it was my job to closely follow and adhere to the cbo, cost estimates, budget forecast coming every report it issued. cbo is what congress relies on, the gold standard. dobson used cbo data and averaged the medicare per beneficiary growth rate from 2010-2013. then he applied that rate to the most recent cbo baseline of medicare spending. his conclusion, medicare spending of the next ten years could drop by as much as $9 billion beyond the cbo
5:16 am

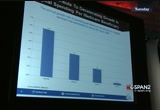
current forecast. this means something, especially after we look under the hood and closely examine the moving parts driving the data. we are now entering the fifth year of record low growth in national health expenditures. the projection for just 13 -- 2013 growth is just under 4%. health care expenditures are continuing their historic slow rate of growth in spite of a slow, but still recovering economy. many are unaware of that dated trans that really hammer home that the -- the spending trend and offers further evidence that the slowdown will be sustained. this stated trend is reflected in a stunning drop in health care prices. health care prices have fallen 6% in 2009 to a near record low of just under 2% last year, the
5:17 am

second lowest level in the last 50 years. when i say prices, i mean the payments for services, not something reflective of the charge master. these are the actual payments for services. hospital price growth which fell by more than half since 2009 to one and a half% in 2013 is leading the way. more evidence of hospitals leading role in slowing health care cost growth is captured in this chart. it shows the steady decline in medicare hospital spending measured on a per beneficiary basis of. look at the bar on the far right in 2012 there was near zero growth in hospital spending. medicare inpatient spending per beneficiary actually declined to estimate to a half percentage. what is going on? what is driving these trans?
5:18 am
james carville many years ago said it is the economy, stupid. now at least in terms of health care is the structure. the slow economy starting with the recession, the great recession does play a role, but dobson knows, new economic research suggests that the economy may have had an even smaller impact on health care spending than thought as recently as one year ago. what matters more and more are the structural changes taking hold in the delivery and financing of health care. this undoubtedly is what the head of the cbo man to and ' did you see here. you see that he references beneficiary and provider behavior as contriving the slowdown and discounts financial turmoil and the recession. i am sure this is no surprise to
5:19 am
any of you. all of you know this. all of you are creating change every day in hospitals through reduced rea admissions, building integrated care networks, the playing sophisticated information technology systems and expanding the use of electronic health records. it is all about efficiency and enhancing values. our mission now should be to stay the course with the structural innovations and the reforms that are driving the slowdown. in so doing we will keep within reach the $900 billion in additional medicare savings that dobson sites. this is why this morning i am sending the dobson report to the house and senate budget committee who will be analyzing the white house budget. i will also send them a letter urging congress to exercise caution and avoid burdensome
5:20 am

policy mandates and a new hospital payment cuts. enough is enough. hospitals already must absorb 117 and a half billion dollars in cuts imposed just since 2010. at the same time the medicare payment advisory commission which advises congress about medicare estimates that medicare margins per hospitals will fall to-8% in 2014. that is an all-time low. let me conclude by making two key points. clearly any further cuts will jeopardize access to care. the second, for it any further cuts it would be it jeopardize of investments hospitals must make to accelerate the structural changes driving the new era of low-cost growth. i encourage you to read there report in full, which you can get access to the a policy
5:21 am

blocks. fah policy. now we will move on in the program. and thank you for your patience with me, senator widen. also, to look back to the high side from bonnie to see whether the center is here. >> he is walking in. he will be here in a moment. in so that gives me a chance to get my notes together. [silence]
5:22 am

>> our first speaker this morning is center ron wyden, the new chairman of the senate finance committee -- i should say the powerful senate finance committee. he has been a public servant in washington for 32 years. he has recently taken the helm as chairman of the senate finance committee, elected to the senate in 1996 and elected to the house of representatives first in 1980. i have known center widen for much of his capitol hill career, and i have always had a deep admiration for him. he has tremendous dedication, i great leader in health care, committed to getting things done, has a willingness to reach across the aisle to seek consensus and if some times
5:23 am

causing his democratic colleagues anxiety, he just tells them that they have to live with it. but what strikes me most about him is the effort that he puts into policymaking. he is all about the details, and he is all about doing whatever it takes to get good policy made by the congress. i can remember in the middle 80's when i was the republican health council on the ways and means committee, sitting in my office one afternoon. i got a call -- the phone rang, and on the other end was congressman wyden. first, as a staffer, i very rarely got calls from congressman. to, i don't remember ever getting a call from a congressman who was not on my committee and i served. three, i don't remember any democratic congressman ever calling me in my entire career on capitol hill. it was quite striking.
5:24 am

that did not quite know what to say. i said yes, sir. then he started into a bill he was working on that you wanted to explain and make sure that i and a step that had some questions for me about what we might think about it. that was striking to me. it was unusual. he is an unusual senator, unusual congressman, and is the kind of person you really want in washington. today marks his maiden speech before a major organization since becoming chairman of the senate finance committee, and we are extremely grateful for him to take time from his schedule to come down and see us here and speak to you this morning. ladies and gentlemen, i want to welcome my friend, the chairman of one or -- ron wyden. [applause]
5:25 am

>> what an inflationary introduction. and chip, thank you. without making this a brocade tossing contest, let me tell you what you already know. you are so lucky to have chipcom who has enormous credibility. there was a reason that i called him back when i was a young congressman and had a full head a fair and rugged good looks. he is a straight shooter, and we are lucky to have him. thank you for that kind introduction. let me start by saying at think it would be cruel and unusual punishment to give you a big filibuster. a lot of you had to brave the elements. i thought what i would do is offer a few thousand particularly well chosen words. my staff wrote this wonderful speech. i can put it in the congressional record and mail it to you, but to give you a little bit of a sense of where i think that we are on health policy and then throw it open to questions.
5:26 am

suffice it to say, most of health policy really is not health policy and all. it is essentially budget policy. and so that congress just ducks on so many of the big issues and then sub putting together something that in the parliaments of washington might be called a patch. maybe it is an extension. maybe it is called a stop gap, but the fact is, it ducks the big issue. it repeatedly ducks the big issue, particularly on medicare when you have 10,000 people eligible for medicare every year -- every day. there is a very real cost attached with the. so now the challenge is to try to find a way to move beyond this sick -- fixation on budgeting. it would be one thing if it was sound budget policy, but so
5:27 am

often as i have indicated we don't get at the structural kinds of issues. and move beyond this sort of large from one kind of budget calamity to another and come up with some sensible budget policies. now, we have an opportunity to begin that with the legislation that, of course, involves reimbursement for physicians, what is called the fg our bill. of course this is enormously important to hospitals as well because you all employ so many physicians. now, finally we have got an opportunity to start moving medicare in the right direction because in effect we are assessing the first real day, the first real date for getting serious about moving away from fee-for-service medicine starting in 2017 as a result of this legislation, providers
5:28 am

would be rewarded for pursuing the delivery model that no longer is built just around fee-for-service medicine. instead, providers in other kinds of coordinates models would have an opportunity to, and in fact, when when they were able to provide better quality versus the old model of volume driven madison. those that decide against participating can continue to practice, but they're not going to have the same kind of financial reward. so in effect it is a pretty straightforward choice. quality care and an advance payment model with the potential for those kinds of financial rewards or basically business as usual, status quo, volume driven kinds of medicine. so in my view, getting a date will we're going to say we're
5:29 am

finally serious about setting aside a fly ball strikes me as a very useful step. it is particularly valuable because of the challenge that i envision for medicare in the days ahead. back when i was co-director of the oregon grape panthers even before i was calling chip nights and weekends when he was a young staffer as well to my we did not have the medicare program that we have today. today medicare is all about crack disease, diabetes, cancer, stroke, heart, that would really dominate all of the spending in medicare, well over 80 percent. the reality is the system has not kept up with it. and if you are having trouble sleeping tonight, we put on our website a kind of detailed explanation of what the challenges, created a person that we call mrs. jones who is
5:30 am

really the typical chronic care patient and is essentially after mrs. jones gets her free physical from medicare, thank you, a cnn that point, the whole system kind of goes off the rails almost until the time where mr. jones will end up in a hospital emergency room with that $1,100 deductible that she has to figure out how to pay and at that point cannot even remember all of the providers that she saw on that odyssey through the health care system. so, the fact that we are now moving with the fg our bill in a coordinated care push means that when we get sg our past and start those incentives for coordinated care when naturally can segue into a better delivery system for chronic care patients
5:31 am

in fact, we really jump-start the effort to pursue more thoughtful policies in the fgr bill because in and the fg our bill this he snips, what are called diachronic special needs plans that have not worked out particularly well, we would also see some improvement in those starting quickly because in the bill we provide that the sea snips would, in effect, start locking in the individual care plans which is so important if you are going to move to a more coordinated model committed to physicians and croupier's and nurses and pharmacists together. so the fgr bill which has has indicated is a big plot in terms of the real date for moving away from fee-for-service also gives us a chance to begin the effort to more coordinated care
5:32 am

services for the chronic care population who, in my view, are going to be with medicare is all about. there is one other part that i want to mention, and we will wrap up with a couple of thoughts on the ac a. senator grassley is a republican senator from iowa. if any folks are out there for my luck will make sure you give a special pad on the back. he and i have been prosecuting the case for opening up the medicare database for many years so that we could get that information of services and providers which has largely been included. my view is when that information becomes public, that, in effect, will be a new base line for health care cost and services in our country because not only will it be a value in the medicare context, but my sense
5:33 am

is anybody who has an employer plan, anybody who has an age as a plan, let's say you live in denver, for example, like the kind of information with respect to building in services and quality that this legislation is going to make more available and transparent. if you have an age as a plan or employer plan you will say, why can't i have that same rate and those kind of benefits that you have with medicare. i think this will be a big plus for the entire health care system, and it has been included let me wrap up with a question -- common to on the dca because, of course, we will be looking at it in the senate finance committee, a variety of issues, oversight with the administration presented its budget. my general approach to this is going to be much like my approach when i voted for george
5:34 am

w. bush's medicare program and medicare part b. i was one of nine democrats who voted in the united states senate. i still have the wealth on my back to show for. there were a lot of friends in the gray panthers days when i worked with seniors to said, wrong, that's it. we're not going to support you anymore. once you do of this bipartisan stuff which is fine. that program is a boondoggle, i give away to bake pharma. he should not have voted for it. that is that. frankly, i cannot recall an occasion where i got more slack. as you know, it has turned out to be an extraordinary success story. they have come in 45%, 45 percent below projected cost. and there really is not anybody
5:35 am

in the congress here now talks about repeal or derailing it. that is because an enormous number of seniors and families have peace of mind and security as a result of making the program work. i bring this up only by way of saying that a lot of the stories a day of the ac a first few months show a remarkable resemblance to the stories about part de in its few months. western civilization is going to hand. the bureaucracy is torturing us. back-and-forth the debate went. what i will try to do on the finance committee is bring the same bipartisan approach that i did in terms of working when a republican president got his major health initiative through and bring that same approach that i used the party to try to work with colleagues in a bipartisan way on the dca as we
5:36 am

move forward. let me use that as a kind of opening salvo. questions are welcome when you're pretty much right off the plan from oregon. thank you for the work they do. you play a pivotal role in the health care delivery system in our country. i've enjoyed working with you in the past. we have a lot to do in the days ahead. i look forward to continuing their relationship. [applause] ..
5:37 am

>> i am supportive of those who comes from a state like oregon. sort of a procedure path on a spell. first of all, i am kind of the parachuting in the last moment. in other words, the discussion was largely conduct did on each side by chairman bachus. the basic lay of the land has been on the procedural aspect of it. still the heavy lifting department in terms of this and a lot of people are automatically saving, where we
5:38 am

going to go forward. in an ideal world if i had my way, we would tackle some of these military weapons system that i don't think are relevant as we generate the savings. and that would be a possible part to pay for it. that's not on the table right now. we have some tough decisions ahead. since i am a newly minted chair, we went right after valentine's day, i spent time with the chairman of the finance committee for leval for days. discussions with the house. i have been supportive of those programs and i am going to continue to be. obviously we're going to have to make a call as for a cost-effective way to pay for them. >> that was a real deal.
5:39 am

>> we have used this last program for $100 billion in programs. these cuts occurred in 2010, they have a real impact on service we provide them jobs as well. as the new chairman, what is your view at hospitals pay for other programs? >> what is striking about it is that it used to be providers had to face tough decisions in terms of taking cuts for health care. and so people would swallow hard and say okay, maybe if we take a hit, elisa goes to benefit the overall health system. at some point i would wash up on our shores in a favorable way. now, we have moved beyond the and health care savings and cuts, essentially being
5:40 am

targeted, goes to entire other areas of the budget as you can probably tell. i'm not holding any rallies for that particular approach. this is going to be a very challenging time. there is no way to pretend anything else. and it used to be that the chairman of the senate finance committee was going to show up and visit with the numbers and had a to the antic and magically pay for this. can probably remember those days when the democratic and republican chairs of the finance committee and the ways and means committee would literally do that. it would be the revenue raisers in our states were a number of years. that is not the way that
5:41 am

budgeting is done anymore. so part of what happens is when you can't make a permanent policy change, which is what i want, i want a family fix from one to another and it provided the certainty that is needed and it's moved away from the fee-for-service and i very much want to address this permanent way. but it does mean that we will have some tough budget calls. and i'm going to do everything i can specifically to make sure that elyse health care reductions aren't used treadmill up another part of the budget. and so it is really fascinating
5:42 am

to see the role of the budget once one all this. it's. >> i just want to take a second, we have always had great bipartisan ideas and prospects for tax reform. what are your prospects for the election? >> cures my sense of where we are. and the chairman is where we are. trying to build on some of the ideas science or do. and he moved in and cleaned out special interest rates to hold down the rate and restoring progress. and what i think the challenge is going to be is to look at where the house and senate turn the table and make at least some
5:43 am

progress in terms of building towards tax reform. what happened last november, and it was widely publicized, is the house leadership essentially said that obamacare was going to be their course for 2014. that is what they were going to put the focus on. and when they do that, that really changed the timetable. so the chairman was still chairman of the senate finance committee. but of course he is retiring in 2014. i had to make some decisions about where we are. even one the chairman talked about how it would affect tax reform.
5:44 am

and so the house and the senate have to deal with something called the tactics standards. and this is about 55 provisions, number of which affects health care. and there are a lot of spenders and involving energy speaking hypothetically with five provisions on energy. two of them would be enough to obtain your objective in part of this to generate the savings so that you're making a jump start to tax reform. now this kind of illustrative of my philosophy, between now and
5:45 am

the election of my pharmacy. there are three major pieces of legislation that have a date stamp on them. this is the republican from new hampshire and they had this date stamp on them and then shortly we will run out of money on the highway trust fund. and you can't worry about so in each of those three areas, the
5:46 am

centers and the transportation, my hope is to use those bills as a springboard to broader reform. if we can make this cost defensive policy with respect to its vendors, that is a jump start to tax reform. and i have to give some of the private sector money off the sideline and get it back to the transportation finance system. and that's a very important time and we have to be concerned about these other judgments that are going to be made my pledges
5:47 am

to work with you on these kinds of issues to try to come up with sensible bipartisan policy and this includes health and transportation, to try to make sure that we see those decisions in the kind of prism that we are doing. and we are using it as a springboard for the broader reform. to be continued. thank you. [inaudible conversations]
5:48 am

[inaudible conversations] >> okay. the senator is in the wings, and he is in our next lineup for the speakers. senator roy blunt is the senator from missouri. he has served in the leadership and it is unusual he was elected to the senate in 2010, before that starting in 1996 he was elected first of in terms as a member of the house representatives. as a member of the house his
5:49 am

colleagues elected him three times to serve as the house majority whip and the republican whip, the second ranking highest republican in the house. he is extremely familiar with health policy or hospital policy i have known the senator since he was in the house and i'm not sure that i ever thanked him for anything other than that day. i remember many years ago around 2001 i was leaving the health insurance association of
5:50 am

america, and he was kind enough to come down to a going away party that my colleagues and the board were having that day. it took me back if he was gracious enough to come downtown and say goodbye to someone. and it just struck me that it reflects an unusual kind of person and a real understanding of the importance of a developing relationship. so i deeply appreciate him and i know that you will appreciate him. so let me introduce senator roy blunt of misery. >> thank you for letting me come this morning. thank you for that generous introduction. in the most important domestic issues which are clearly the health issues and we need a lot of python and understanding the
5:51 am

real world circumstances and when it might be. and i'm on the other side of the aisle, i ranking democrat on that side. but ron wyden is a person who reaches out and too many people hold it, if i don't give 100% of what i want, i just assume not have anything, which is almost certain not to get anything. and we the that happens day after day.

5:53 am

i had to come up with alternatives, and at some point in that, i said we could claim some victory if by the time we were done every member in the house knew the difference between medicare and medicaid. [laughter] i'm pretty sure every member of the house and senate does know the difference in in medicare and medicaid, but that was not the case necessarily when we entered this debate. you'd be better at it, we would be better at it, and the country would be insistent we figure out how to do this the right way, and i firmly believe surely we would not in a blanket bill try to manage everybody's health care coverage in a new way and restructure 16 or 17% of the economy. now, whether we can get back to the appointment or not, i don't know, but i know it's a better debate if we did. i also know that some sort of instrumental implementation would have been a better thing, and i introduced the bill in the
5:54 am
house that kept 3 million people on their parents' insurance a little bit longer, and there's some people who criticize that and say, oh, that's the slacker provision. these are people that don't want to pay for insurance, and, you know, the truth is that every state let people stay on their parents' ininsurance, and others like them stay on their insurance until 23, and i had a bill at 25, administration picked it up, and put it in that 26 00-page bill to make it 26 instead of 25, and took a largely uninsured group and moved them from the uninsured column to the insured. senator reid said a fourth of the people got health care that didn't have it before the passage of this bill were people who were now op their parents' insurance. i got the bill back out. i wantedded to see the bill introduced. it was three and a third pages.
5:55 am

i should have introduced 14 pages and had everybody covered. three and a third paging very simple, straightforward, probably insured 3 million people not insured before, but the question i would have is what about the other 2597 pages or whatever is in the 2600-page bill, the law of unintended consequences having big impact now. i met with the hospital executives in st. louis, missouri days ago and said the fastest growing unpaid debt group is now among the insured with high deductibles. deductibles so high frankly that many cannot pay it, and so that sliver of health care is a problem. it is a bigger problem, has been before, because deductibles are higher than they have been before to get the same coverage
5:56 am

and expand this to coverage you or your family don't need, deductible had to go up and often premiums go up as well. these are critical issues, issues we have to deal with, and i want to talk just a little bit about the medicare issues that need to be dealt with and what we can do to deal with them, certainly, i was concerned as were 379 -- 39 of my colleagues, signing a letter to the president and cmh before the medicare advantage cuts were announcedded or as they were announced, and don't cut the program anymore. adopt make it harder anymore for people to supplement insurance or make it harder in a noncompetitive marketplace to have competitors to allow them it pay that part of the bill. i think what will happen is you
5:57 am

reduce medicare advantage, you'll see seniors that are not covered that are currently covered. you'll see prescription premium increases and a lot of seniors are not going to have this coverage that they had before. this is where the market place actually in helping to create a market place rather than create a system is a place where the government does good. we saw that in medicare part d. it was the first program in health care that the government ever -- the federal government ever got involved in where the goal was not to operate a system but create a market place, and to see that happen and see like the early results at least until recent changes, i don't know what the changes mean, but medicare part d came in year after year 40% lower than the lowest possible estimate of cost than when the bill was passed because the marketplace can and does work.
5:58 am

medicare bad debt is another area where if we think there's no impact on hospitals and health care providers, we are making a big mistake, and we need to continue to look at medicare bad debt. it shouldn't become a pay-for for other health care services. i think we have to be very thoughtful that we understand that medicare bad debt is a program for hospitals that are already operating on narrow margins, and we don't need to make those margins so narrow that hospitals can't stay in existtense leading me to rural hospitals. the rural hospitals extending medicare dependent hospitals and low volume payments through the end of the fiscal year. we have to be thoughtful if we think we're going to move into a different environment next year where rural hospitals don't need
5:59 am

that kind of assistance. i was pleased to be the principle response sore of the medicare audit improvement act. sometimes this is called the rack, and from the middle ages until about 17 # 00 in europe. the rick was widely used, and the purpose was just to stretch you until you timely admitted whatever had to be admitted so they stop stretching the rack, and seems to me there's an awful lot of that principle in the recovery audit program where the recovery audit program, particularly for small hospitals or hospitals that can't just perm inaptly have somebody or a team dedicated to this do not fight back, and even if they do, the fight takes so long that it appears over and over again the goal of the federal government is to get you to give up or get you to negotiate quickly to get it over with, and unfortunately,
6:00 am

generally, in the settlements whether it's here or other federal agencies, is the very aggressive stand early in the discussion. we have more time, more lawyers, and more money than you do settle or continue to fight? we have to look at this and be sure that nobodiments taxpayer money wasted or spent in fraudulent ways, but there's a better way than how we pursue now to see that that doesn't happen. another issue that you worked on as you are more and more impacted by doctor compensation is the sgr. i think we
60 Views
IN COLLECTIONS
CSPAN2 Television Archive
Television Archive  Television Archive News Search Service
Television Archive News Search Service 
Uploaded by TV Archive on
